
New definition of Diabetic Ketoacidosis (DKA): Coding, auditing, and CDI professionals take note

")
By Brian Murphy
The clinical definition of diabetic ketoacidosis (DKA) is changing. CDI and coding professionals take notice.
A recent article on Medscape (link below) says a forthcoming definition will “de-emphasize glucose from the diagnostic criteria for DKA, along with many other updates to the last statement on the topic, which was published 14 years ago.”
14 years since the last update? I guess we’re due.
The forthcoming statement is authoritative, jointly endorsed by the American Diabetes Association (ADA), the European Association for the Study of Diabetes, the American Association of Clinical Endocrinology, the Diabetes Technology Society, and the Joint British Diabetes Societies for Inpatient Care.
The previous consensus statement on the subject was established by the ADA alone. I have to think this will become the new national (and international) standard.
Per Medscape, for all patients with hyperglycemic crisis, the hyperglycemia cutoff is now lowered to 200 mg/dL (11.1 mmol/L) from the previous 250 mg/dL. It also removes the glucose cutoff entirely for people with a history of diabetes. The new statement classifies DKA by mild, moderate, and severe, but for the first time will offer care recommendations for each level, too.
As I always note in these types of posts I’m not a clinician so I’ll leave it up to others as to how substantial these changes are, from a clinical perspective.
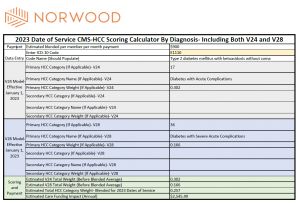
DKA is captured using several different codes but one of the most common is ICD-10-CM code E11.10 (Type 2 diabetes mellitus with ketoacidosis without coma). It’s an MCC in IPPS.
E11.10 also adds weight in both version 24 and version 28 of CMS-HCCs, which are both in play at the moment. So you need to get this captured accurately for basically every major payment model (and of course, for clinical accuracy, which should go without saying).
My colleague Jason Jobes has done some wonderful posts on the HCC changes and financial impacts, and I thought this clinical update dovetailed nicely. The associated table is his.
Note: Just because a definition is changing in the clinical literature it doesn’t mean your physicians will immediately adopt it. It can take months, or longer. Sepsis-2 vs. Sepsis-3 continue to be debated today, for example, and Sepsis-3 debuted in 2016.
But there is a much higher likelihood that insurance companies and auditors will exploit this advantage and deny the diagnosis on the basis of the new criteria. So it behooves your physicians to have the latest and greatest info.
Medscape is a really good resource for this type of information, BTW.
Reference
Medscape, “New Hyperglycemia Emergency Guidance Updates DKA Definition”: https://www.medscape.com/viewarticle/997186
Related News & Insights
Two reasons why the 2027 OPPS proposed rule hurts your hospital
By Brian Murphy The 2027 OPPS (outpatient) proposed rule landed just prior to the July 4…
You should be billing G2211 in heavy volume, per CMS
Who remembers G2211? Starting in 2024 this CPT code took the mid-revenue cycle by storm. Despite paying…